
If your gut issues started after food poisoning, a stomach bug, or getting sick on vacation… that was probably not a coincidence. I work with so many people who were told, “It will pass, give it time.” But years later, they are still struggling with bloating, constipation, diarrhea, fatigue, and digestive symptoms that all started after that one infection. Sometimes the infection leaves… but the damage it creates lingers much longer.

As a Registered Dietitian specializing in IBS and SIBO, one of the most common root causes I see of SIBO is food poisoning. The problem is not always the infection itself. It is the damage that infection can leave behind. When the migrating motor complex gets disrupted, your small intestine loses part of its ability to clear bacteria effectively, and that dysfunction can become one of the driving factors behind SIBO.
What Actually Happens During Food Poisoning
Food poisoning starts when pathogens enter your GI tract and release toxins that damage the gut lining. The acute illness at the time of exposure is vomiting, diarrhea, cramping, fever because your immune system fighting off the infection. For most people, the surface symptoms clear within a few days. The problem though is what may be left behind.
The bacterial pathogens most commonly linked to post-infectious SIBO include:
- Campylobacter — undercooked poultry, raw or unpasteurized milk, and contaminated water.
- E. coli (especially Shiga toxin-producing strains) — undercooked ground beef, raw leafy greens like lettuce and spinach, unpasteurized dairy or juice, and contaminated drinking water.
- Salmonella — undercooked poultry and eggs, raw produce, and unpasteurized dairy.
- Shigella — contaminated water and food handled by an infected person, often spread in close-contact settings like childcare or travel.
- Vibrio — raw or undercooked seafood, particularly oysters and sushi.
- Yersinia — undercooked pork and contaminated water.
Several of these pathogens, particularly Campylobacter, E. coli, Salmonella, and Shigella, produce a toxin called cytolethal distending toxin B (CdtB), the trigger behind the autoimmune mechanism we need to pay attention to.
Even after the infection resolves, the inflammation and damage to the gut wall can linger far longer than the acute illness. A systematic review and meta-analysis found that around 1 in 10 people who experience acute gastroenteritis go on to develop ongoing GI symptoms, a condition called post-infectious IBS (Klem et al., Gastroenterology, 2017). A significant portion of those cases turn out to be SIBO.
Meet the Migrating Motor Complex (MMC)
To understand why food poisoning leaves such a lasting footprint, you have to understand the migrating motor complex, often shortened to the MMC. The MMC is a wave of muscle contractions that sweeps through your small intestine between meals, during a fasting state (Deloose et al., Nature Reviews Gastroenterology & Hepatology, 2012). Its it essentially the housekeeper of the gut, clearing food debris, dead cells, and bacteria out of the small intestine and into the large intestine where they belong.
Think of the MMC as your gut’s cleansing wave. When it is working properly, the small intestine stays the low-bacteria environment it is supposed to be. When the MMC slows down or stops firing, that housekeeping stops. Bacteria that should keep moving through get a chance to settle in, multiply, and overgrow.
Migrating Motor Complex Phases
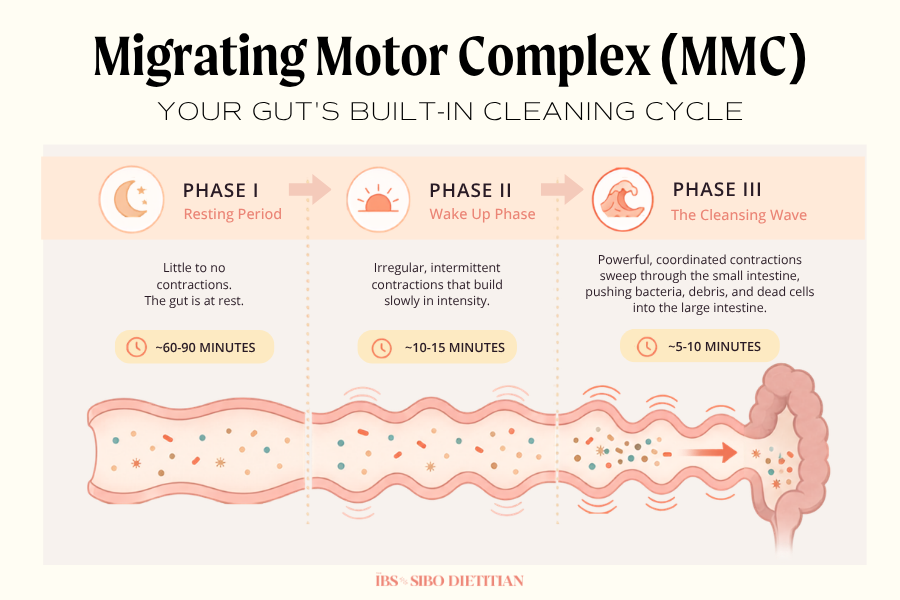
The MMC actually moves through three distinct phases as it completes each cycle. It takes approximately 90-120 minutes to complete an entire cycle:
- Phase I is the resting period, with little to no contractions. This phase makes up approximately 60-90 minutes.
- Phase II is a stretch of irregular, intermittent contractions that build slowly in intensity. This takes about 10-15 minutes.
- Phase III is the cleansing wave itself — powerful, coordinated contractions that sweep through the small intestine for about 5–10 minutes, physically pushing bacteria, debris, and dead cells into the large intestine.
- Phase IV is the transition cycle, a brief wind-down period where the phase III contractions taper off and start back at phase I.
Phase III is the piece that actually does the housekeeping work. When food poisoning damages the MMC, Phase III contractions weaken or stop firing altogether. Without that sweep, the small intestine loses its built-in defense against bacterial overgrowth.
It is important to note, the moment that you consume something caloric, whether it is liquid or food, the cycle restarts at phase I. This is why meal spacing to supporting the MMC can be one of the most powerful things you can do to ensure the cycle reaches Phase III.
This is one of the most underappreciated pieces of the SIBO healing puzzle. Most providers focus on the overgrowth itself (what is growing, what to kill, what to eliminate) without ever addressing why the bacteria are there in the first place. The answer very often traces back to motility, and the MMC is the engine that drives it.
How Food Poisoning Damages the MMC: The Autoimmune Connection
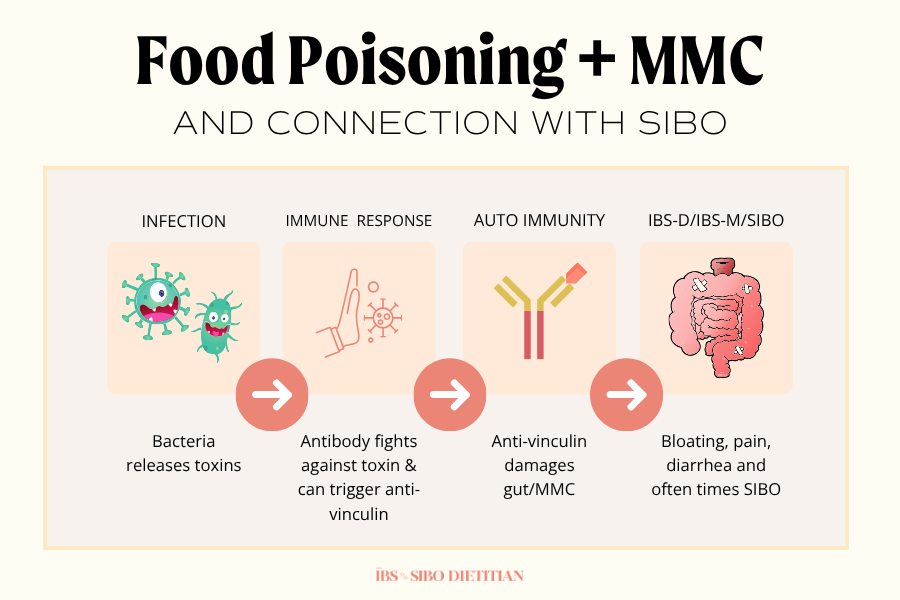
Here is where things start to connect. When the bacteria that cause food poisoning multiply in your gut, they release a toxin called cytolethal distending toxin B, or CdtB as mentioned earlier. Your immune system creates antibodies against CdtB to neutralize the infection. The problem is that CdtB looks structurally similar to a protein in your gut called vinculin, which lives inside the interstitial cells of Cajal, the pacemaker cells responsible for triggering MMC contractions.
In a subset of people, the immune system cross-reacts. The antibodies it built to fight CdtB end up attacking vinculin too. This is molecular mimicry, and it sets off an autoimmune process that damages the very cells that drive your gut’s cleansing wave (Pimentel et al., PLOS ONE, 2015). The infection resolves, but the autoimmune damage continues quietly in the background.
This research comes out of Dr. Mark Pimentel’s lab at Cedars-Sinai, and it changed how we understand post-infectious SIBO. His team developed the IBS-Smart blood test, which measures anti-CdtB and anti-vinculin antibodies and helps confirm whether an autoimmune mechanism is driving someone’s SIBO or IBS-D. When those antibodies show up elevated, it points directly back to a prior infection, even one the person may not remember clearly.
What this means clinically is significant. Food poisoning does not just inflame your gut temporarily. In some people, it sets off an ongoing autoimmune attack on the system that prevents SIBO. The acute illness ends, but the motility damage does not.
The Transition From Post-Infectious Gut to SIBO
Once the infection itself clears, this is usually when symptoms begin to slowly change.
At first, it may just feel like your digestion has not quite gone back to normal. You notice more bloating, especially as the day goes on. Bowel movements become inconsistent. Foods you used to tolerate without any issue suddenly feel harder to digest, leave you feeling overly full, or trigger symptoms that never used to be there.
Common symptoms that often begin showing up include:
• Bloating that worsens throughout the day
• Increased gas or visible distension after meals
• Constipation, diarrhea, or alternating bowel patterns
• New food intolerances or increased food sensitivities
• Fatigue or brain fog that seems disconnected from digestion
What most people do not realize is that the infection may be gone, but the effects it left behind can remain.
One of the biggest concerns after food poisoning is damage to the migrating motor complex, which is the system responsible for creating cleansing waves in the small intestine between meals. Its job is to move leftover debris and bacteria down through the digestive tract so they do not accumulate where they should not be.
When that process becomes impaired, bacteria begin building up in the small intestine. As bacteria accumulate, fermentation increases. More fermentation leads to more gas production, more distension, and further slowing of motility, which only continues feeding the cycle.
Signs Your SIBO May Be Post-Infectious
Not every case of SIBO traces back to food poisoning, but several signals make a post-infectious origin more likely. If most of these sound familiar, the post-infectious pathway is worth exploring with your provider.
You may have post-infectious SIBO if:
- You can pinpoint a specific GI illness — food poisoning, traveler’s diarrhea, a stomach bug — that preceded your symptoms.
- Your symptoms came on suddenly rather than building gradually over years.
- You developed bloating, diarrhea, or irregular bowel movements within weeks or months of being sick.
- You have done a round of antibiotic or herbal treatment, and your symptoms temporarily improve but come back.
- A provider has labeled your symptoms as IBS-D or post-infectious IBS.
- Your gut has never felt the same since “that one trip” or “that one meal.”
- Your bloating worsens the longer you go between meals, briefly improves with eating, and escalates again as the day goes on.
If several of these resonate, the post-infectious mechanism is worth confirming through testing rather than continuing to chase symptoms.
What to Do If You Think Your SIBO Started With Food Poisoning
If your SIBO started with food poisoning, your treatment plan needs to look different than a generic SIBO protocol. This is not a case of clearing the overgrowth once and moving on, because the underlying driver, impaired motility, is still there, ready to let SIBO right back in.
A more effective approach addresses all four layers together:
- Confirm post-infectious SIBO with testing. A lactulose breath test identifies your subtype (hydrogen, methane/IMO, or hydrogen sulfide), and the IBS-Smart blood test confirms whether anti-CdtB and anti-vinculin antibodies are driving the picture. While testing for antibodies isn’t a crucial step, it can give you data on root cause.
- Clear the overgrowth. This may involve rifaximin (and neomycin if methane is present), herbal antimicrobials, or a combination, depending on your subtype and history.
- Restore motility. This is the piece most providers skip entirely. Prokinetic agents, meal spacing of 4–5 hours between meals, magnesium, and vagus nerve support all help rebuild MMC function.
- Prevent recurrence. Post-infectious SIBO tends to have higher recurrence rates because the autoimmune damage continues even after the bacteria clear. It is still unclear how long you will posess these antibodies. Long-term motility and nervous system support are essential, not optional.
Treating post-infectious SIBO without supporting the MMC is like pulling weeds without removing the roots. You might see temporary improvement, but the problem was never fully addressed.
How to Lower Your SIBO Risk After Food Poisoning
The acute phase of food poisoning is hard to ignore, but the days and weeks afterward are when SIBO can develop. The window to support your gut and reduce your risk of progressing to post-infectious SIBO is right after the infection clears, not months later. If you have just been sick or suspect a recent food poisoning, these are the steps I would consider, especially if you have a personal history of SIBO and want to avoid relapse.
- Saccharomyces boulardii. This is a probiotic yeast with strong research behind it for infectious and antibiotic-associated diarrhea. It supports the gut barrier, competes with pathogens, and is generally well-tolerated even when other probiotics are not (McFarland, World Journal of Gastroenterology, 2010).
- Short-term antimicrobials like oregano oil. Used briefly, oregano oil and other botanical antimicrobials can help reduce bacterial load. This is short-window support, not a long-term protocol.
- Binders, used early. Activated charcoal or bentonite clay can bind bacterial toxins in the acute phase, especially within the first 24–48 hours. Take them away from food, medications, and supplements to avoid binding the wrong things.
- Electrolytes and hydration. Diarrhea and vomiting deplete sodium, potassium, magnesium, and chloride quickly. Replenishing them supports motility, energy, and recovery — more on this in my post on electrolytes and IBS.
- Fermented foods, cautiously. Once the acute illness clears, small amounts of well-tolerated fermented foods like sauerkraut, kefir, or yogurt can help rebuild microbiome diversity.
- Get tested if symptoms linger. If bloating, irregular bowel movements, or fatigue continue beyond two to three weeks after the illness, do not wait it out. The earlier post-infectious SIBO gets caught, the easier it is to treat before it becomes chronic.
This is one of the only points in SIBO care where early action can change the entire trajectory. Most clients I see arrive years after the infection. However, people who intervene early are often the ones who avoid the long road of chronic SIBO altogether.
How I Work With Post-Infectious SIBO
I build my approach around the understanding that motility, not the overgrowth itself, is the central problem in post-infectious SIBO. Antibiotics and herbal protocols almost never hold long-term without addressing the MMC underneath.

Working with me 1:1 typically includes:
- A thorough intake that maps your timeline back to the original trigger, even if it happened years ago.
- A testing plan that confirms both the SIBO subtype and the post-infectious autoimmune piece when relevant.
- An individualized food, motility, and lifestyle plan built around your specific picture.
- Prokinetic and nervous system support tailored to your physiology and tolerance.
- Ongoing sessions to clear the overgrowth, walk through reintroduction, and rebuild gut resilience.
- A long-term recurrence-prevention plan, because post-infectious SIBO almost always requires one.
- A clear plan that gives your body the foundations it needs to succeed, so you are not just chasing symptoms, but rebuilding the system that has been damaged.
The goal is not another round of antibiotics or another restrictive diet. The goal is to repair the underlying motility and give your gut the conditions it needs to actually heal.
The Bottom Line
Food poisoning is one of the most common and overlooked triggers of SIBO. The mechanism is specific and well-researched. A bacterial toxin sets off an autoimmune process that damages the MMC, and once that cleansing wave stops working, bacteria build up in the small intestine and SIBO takes hold.
If you can trace your symptoms back to a specific infection, you are not imagining the connection. Your gut is telling you something real, and the right care addresses the motility piece directly instead of just chasing the overgrowth around in circles.
If this sounds like your story, I would love to talk.






