
If you have been bloated for so long that you don’t even know what is normal anymore, you are not alone.
While bloating can present itself in different ways, so many of my clients describe the same experiences. They either wake up bloated, or they wake up flat and watch their stomach grow throughout the day, or they get distended after every single meal no matter what they eat. But the common denominator is that they “don’t remember a time” when they are not bloated. They have been told to drink more water, stress less, cut out gluten, take a probiotic, and that everything looks “normal”. Meanwhile, they have already eliminated half their diet, tried all the supplements, and they are still bloated.

As a Registered Dietitian specializing in IBS and SIBO, here is what I want you to understand. Chronic bloating is almost never normal, despite the normal lab values. The pattern of your bloating can give you more insight than any lab work can. Once you learn how to read it, the answer becomes clearer and helps give you a much more solid plan on how to manage it.
What Is Your Bloating Actually Telling You?
When a client tells me they are bloated all the time, I am not asking what they ate first. I am asking four very specific questions:
- Where is the bloating?
- What time of day is it worst?
- What is happening surrounding your meals (mood, stress level)?
- And how are your bowel movements?
Those four pieces usually tell me what is going on before we change a single thing about their diet.
Bloating is a symptom, not a diagnosis. The pattern of when and how it shows up is the most important diagnostic clue you have. Different patterns point to different mechanisms — motility, fermentation, digestion, hormones, or the nervous system (Lacy et al., American Journal of Gastroenterology, 2021). The only way to fix it is to address the right one.
There two main pieces to decoding your bloating is where it is showing up, and when it is showing up.
Where Is Your Bloating Located?
Before we even talk about timing, the location of your bloating is one of the fastest clinical clues you have. Where you feel and see distention on your abdomen tells me which part of the digestive tract is struggling, because different organs sit in different zones, and bloat in different places for each.
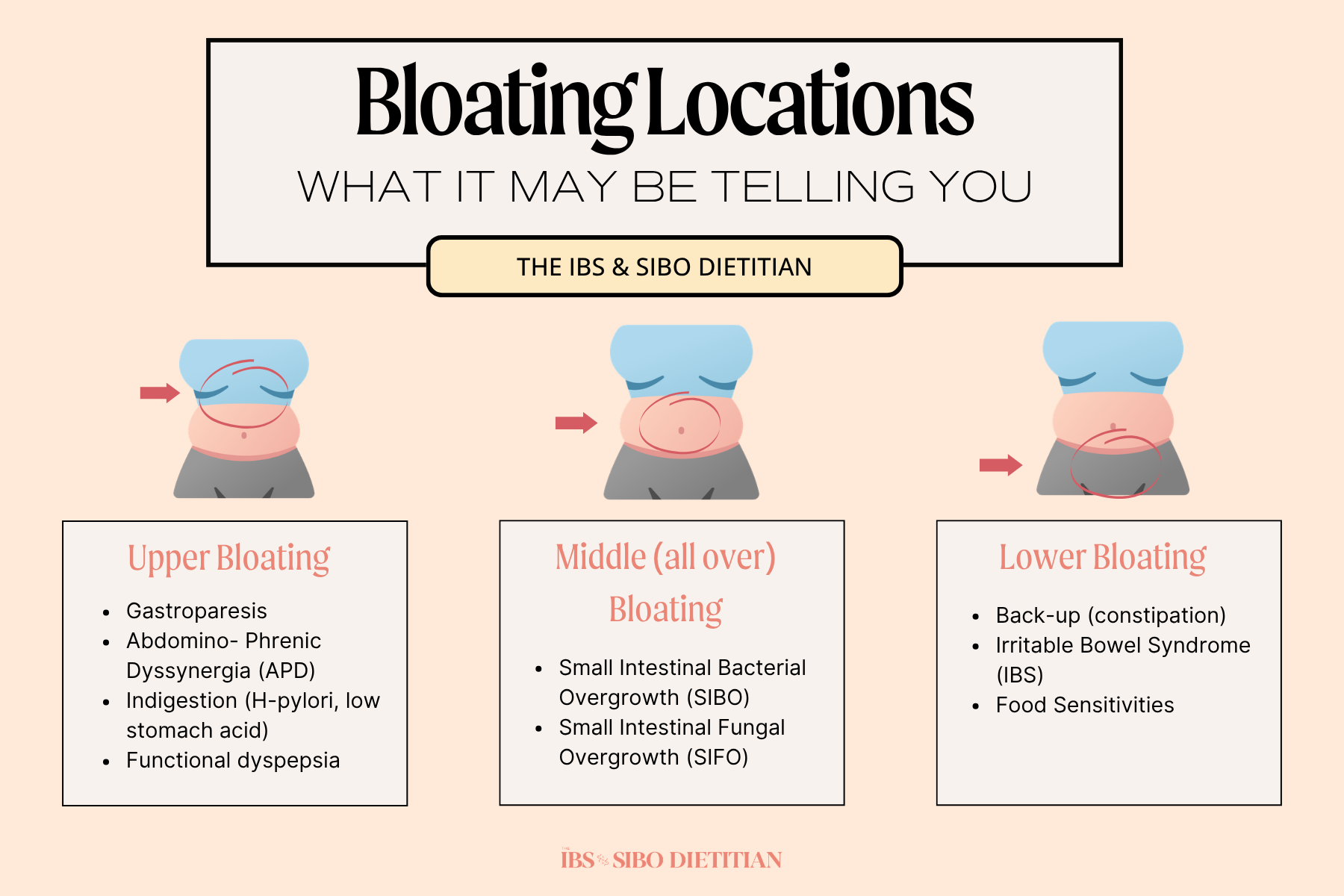
Upper Bloating
If your bloating sits high, under your ribcage (epigastric area), or feels like fullness right after a few bites of food, the issue is almost always at the top of the digestive tract or your stomach. This pattern is a sign that your body is struggling in with gastric emptying or digesting efficiently.
The most common drivers I see in this zone are:
- Gastroparesis (delayed stomach emptying)
- Abdomino-phrenic dyssynergia (a coordination issue between the diaphragm and abdominal wall)
- Indigestion related to low stomach acid or low enzyme production
- H. pylori
- Functional dyspepsia (Stanghellini et al., Gastroenterology, 2016). Clients with upper bloating often describe early fullness, nausea, reflux, or feeling like food is “just sitting there” after a meal.
Clients with upper bloating often describe early fullness, nausea, reflux, or feeling like food is “just sitting there” after a meal. This pattern almost never improves with FODMAP elimination because the issue is not in the colon.
Middle or All-Over Bloating
If your bloating feels like it takes over your whole abdomen, more of that round, “6 months pregnant looking by the end of the day” that is likely your small intestine talking. The small intestine is the longest section of your digestive tract, and when something is going wrong here, the bloating tends to look diffuse and “everywhere” rather than concentrated in one spot.
The two biggest drivers in this zone are
- SIBO (small intestinal bacterial overgrowth)
- SIFO (small intestinal fungal overgrowth)
Middle / all-over bloating is one of the strongest clinical signals to consider breath testing rather than another round of dietary restriction. (Pimentel et al., American Journal of Gastroenterology, 2020).
Lower Bloating
If your bloating sits below your belly button, a heaviness or pressure in your lower abdomen, often paired with bowel symptoms, the issue is often in the colon.
This is the classic location for constipation-driven bloating, IBS, and food sensitivities or fermentation in the large intestine.
This is the classic location for:
- Constipation-driven bloating
- Irritable Bowel Syndrome (IBS)
- Food sensitivities (FODMAPs)
- Fermentation in the large intestine or dysbiosis
Lower abdominal bloating often goes hand in hand with incomplete evacuation, hard or pellet-like stools, alternating constipation and diarrhea, or significant gas later in the day. The colon is where stool sits, where final fermentation happens, and where IBS most commonly expresses itself (Lacy et al., American Journal of Gastroenterology, 2021). If your bloating is concentrated low and your bowel movements are not consistent, this is your colon waving a flag.
Once you have a sense of where your bloating is sitting, the next layer of the puzzle is when it shows up. This is where the timing patterns come in.

Patterns to Look For with Bloating
Now that we have discussed the places where bloating exists, I want to now talk about the patterns. Because the patterns of your bloat can point us in the direction of how to treat your bloating.
Pattern 1: Back-Up Bloat (Constipation)
This is the pattern where you wake up already bloated and watch it progressively worsen as the day or days goes on, often only easing once you finally have a full bowel movement.
Now you may be saying, “I poop every day so I can’t be constipated.” However, constipation is not just about frequency. According to the Rome IV criteria, constipation is defined not just by frequency, but by stool consistency (hard or lumpy stools), straining, incompleteness of evacuation, a sensation of blockage, or needing to manually assist (Bharucha & Lacy, Gastroenterology, 2020).

Causes of Back-up Bloat
Stool that sits in the colon overnight continues to ferment, produces gas, and stretches the colon wall, which is why so many people wake up feeling just as, if not more, bloated than before they went to bed. When your colon does not fully clear, gas accumulates overnight. By morning, you wake up with a hard, distended abdomen, often before you have eaten a single thing.
Common drivers include:
- Low fiber intake
- Inadequate hydration
- Low mineral status (particularly magnesium and potassium)
- Sedentary lifestyle
- Nervous system dysregulation
- And certain other conditions such as thyroid, intestinal methanogen overgrowth (IMO), etc.
Pattern 2: Fermentation Bloat (Diurnal)
Diurnal bloat (often referred to as evening bloating) refers to a common pattern where a person wakes up with a flat or normal-sized belly that progressively becomes larger and more distended as the day goes on. Clients describe waking up with a flat belly and after the first sip of a drink or bite of a meal, the bloat looks as if you are visibly 6 months pregnant.

Causes of Diurnal Bloating
This is the pattern I see most often in practice, and it is one of the strongest clinical clues for SIBO (small intestinal bacterial overgrowth) or IMO (intestinal methanogen overgrowth). In a healthy gut, the small intestine is meant to be relatively low in bacteria. In the case of SIBO, bacteria that should be present in the large intestines, becomes overgrown in the small intestines. When too many bacteria, or specific methane-producing organisms, overgrow in the small intestine, the food you eat becomes the bacteria’s preferred fuel. In turn, the byproduct is gas. This gas continues to build with each meal, and because the migrating motor complex (the cleansing wave between meals) is often impaired, that gas does not get cleared efficiently (Pimentel et al., American Journal of Gastroenterology, 2020).
Common drivers include:
- Impaired or slowed motility
- Migrating motor complex dysfunction
- Small intestinal bacterial overgrowth (SIBO)
- Intestinal methanogen overgrowth (IMO)
- Small intestinal fungal overgrowth (SIFO)
- Post-infectious gut dysfunction (food poisoning, prior GI infection)
Pattern 3: Digestive Bloat (Post Meal)
Digestive bloat refers to a pattern where the bloat shows up shortly after eating or drinking, often within minutes. Clients describe a heavy, “brick in the pit of the stomach” feeling that comes on as soon as they start a meal. The bloating tends to sit high in the upper abdomen, and is often paired with reflux, burping, or a sense that the food is just not moving down.
Causes of Digestive Bloating
This pattern is almost always pointing to something happening at the very beginning of the digestive tract, rather than further down in the small or large intestine. When the stomach is not producing enough acid, or your body is not effectively producing digestive enzymes, food sits in the stomach longer than it should and begins to ferment early. The result is upper abdominal pressure, gas, and that classic post-meal heaviness within minutes of eating (Mayo Clinic, 2024).
Common drivers include:
- Eating too quickly
- Swallowing air (talking while eating, gum chewing, drinking through straws)
- Carbonated beverages
- Low stomach acid
- Digestive enzyme insufficiency
- H. pylori infection
- Functional dyspepsia
Pattern 4: Hormonal Bloat
Hormonal bloat is a cyclical pattern commonly seen in women, where bloating peaks in the days leading up to and during menstruation, and then improves once the cycle moves forward. For many women, this shows up as a noticeable shift in the second half of their cycle, where digestion slows, water retention increases, and the abdomen feels heavier and more distended than usual.
Causes of Hormonal Bloating
This pattern is driven by the natural fluctuations of estrogen and progesterone throughout the cycle. Higher estrogen levels (especially relative to progesterone) can drive water retention and increase visceral sensitivity, making the same amount of gas feel significantly more uncomfortable than at other points in the cycle. At the same time, progesterone slows gut motility in the luteal phase, which is why so many women experience constipation, gas, and bloating in the days before their period (Heitkemper & Chang, Gender Medicine, 2009). For clients with underlying IBS or SIBO, the luteal phase often acts as an amplifier, making symptoms that were already simmering get loud during this window.
Common drivers include:
- High estrogen relative to progesterone
- Impaired estrogen clearance (often tied to gut and liver health)
- Low progesterone
- Mineral depletion (particularly magnesium)
- Underlying IBS, SIBO, or constipation that gets amplified during the luteal phase
Pattern 5: Functional Bloat (Nervous System / Visceral Sensitivity)
Functional bloating is the pattern with no clear pattern. Bloating shows up frequently, but it does not track consistently with meals, time of day, hormones, or specific foods. Clients often describe feeling bloated “all the time” or “for no reason,” and find that standard interventions like diet changes, supplements, and even successful SIBO treatment only partially help.

Causes of Functional Bloating
This pattern is largely driven by the nervous system and visceral hypersensitivity. The vagus nerve, which controls stomach acid release, enzyme secretion, and gut motility, is often underactive in this group, which means digestion is being asked to happen in a sympathetic, fight-or-flight state instead of a calm, parasympathetic one (Breit et al., Frontiers in Psychiatry, 2018). On top of that, the gut itself becomes hypersensitive, meaning normal amounts of gas, food, or fluid in the GI tract are perceived as painful, distending, or abnormal. This is one of the most common findings in IBS and is rarely caught with standard testing.
Common drivers include:
- Chronic stress and a dysregulated nervous system
- Poor vagal tone
- Visceral hypersensitivity (often seen in IBS)
- Trauma history
- Eating in a sympathetic, “on the go” state
Pattern 6: Food Intolerance Bloat
Food intolerance bloating is generally tied to a specific food or category of foods, and is a pattern that often gets confused with food allergies. Unlike true food allergies, which tend to produce immediate, often histamine-driven reactions, food intolerance symptoms usually show up hours after eating, sometimes not until later in the day or overnight. Symptoms commonly include bloating, abdominal pain, diarrhea, gas, and nausea, which makes the trigger food difficult to identify without a structured approach.

Causes of Food Intolerance Bloating
Food intolerance bloating happens when a particular food cannot be properly digested or absorbed, leading to excessive gas production, water shifts in the gut, or inflammation in the GI tract. The most common offenders are lactose, fructose, gluten, and FODMAPs (Tuck et al., Nutrients, 2019). One important nuance: food intolerances are very often a downstream issue rather than a primary one. SIBO, low enzyme output, and gut dysbiosis can all create intolerances that did not exist before, which is why simply removing the food long-term rarely fully resolves the issue.
Common drivers include:
- Lactose intolerance (low lactase enzyme)
- Fructose malabsorption
- Gluten or wheat sensitivity
- FODMAP sensitivity
- Underlying SIBO or dysbiosis driving secondary intolerances
- Low digestive enzyme output
So What Is Normal Bloating?
Not all bloating is a problem. Some bloating is a normal part of digestion, and knowing the difference between normal and abnormal helps you figure out when something actually needs attention.
Normal bloating is mild, short-lived, and tied to a clear cause. Gas from fiber fermentation, for example, is a sign your microbiome is doing its job (Cleveland Clinic, 2024).
Normal Bloating
- A little fullness or distention after a large meal
- Mild bloating after a high-fiber meal with beans, lentils, or cruciferous vegetables
- Slight bloating in the days leading up to or during your period
- Transient bloating that resolves on its own within a few hours
- Bloating that fully clears with a bowel movement
- Occasional bloating after a high-sodium or restaurant-style meal
Abnormal Bloating
- Bloating that is constant or shows up daily
- Bloating that is painful or causes significant discomfort
- Distention that dramatically changes the shape of your abdomen
- Bloating that lasts all day, every day, regardless of what you eat
- Bloating paired with reflux, fatigue, brain fog, or hormonal symptoms
- Bloating with irregular bowel movements (constipation, diarrhea, or alternating)
- Bloating that drives food fear or constant restriction
Daily bloating is a signal something is off, and it deserves more attention than “just cut out gluten.”
The Bottom Line
If you are always bloated, the answer is rarely one more food to remove. Your bloating is almost always pointing to something specific, whether it be motility, fermentation, digestion, hormones, or your nervous system, and the pattern tells you which one.
Once you know which pattern you are dealing with, you can stop eliminating foods and start addressing the actual mechanism. That is when bloating finally shifts.
If this sounds like your experience, you do not need another diet. You need someone looking at the full pattern with you.
More on the Blog
- Why Work With a SIBO Dietitian? What They Do and When You Need One
- Is Flaxseed Low FODMAP? Dietitian’s Guide to Flax for IBS and SIBO
- Why Am I Bloated? What Your Bloat Pattern Is Telling You
- Electrolytes and IBS: Do You Actually Need Them?
- Low Ferritin and SIBO: Why Iron Levels Remain Low







2 Responses
I have all 3 bloating, upper, everywhere and lower….all the time. Upper only happens sometimes if I have a drink or eat. The all over is continuous, but more severe after eating, having alcoholic drinks ( once or twice a month) but especially after a workout.
The lower is full, constant and painful.
I can’t find anyone to help, I’ve seen doctor after doctor, specialist after specialist, had test af5rr test after test….5 years later it gerls like I’m in a nightmare and I just don’t enjoy l8fe anmyore. Going on trips or leaving the house overnight fuels me with anxiety cause I know I’ll flare up severely and I just want to be home.
How do I find someone like yourself to help with this? This article gave me hope, but at the same time I feel defeated because I can’t find anyone locally that seems to have a clue what to do.
I’m a male BTW, I realize this is aimed at women but my symptoms are so severe I can jump 3 shirt sizes overnight, or same day.
I am happy that it provided you with hope! The group programs are woman only but I have limited spots in my 1:1 programs as well as the self study Bloating Breakthrough Academy fo everyone.